Giving hope to those affected
by secondary breast cancer
Research. Support. Education.
Giving hope to those affected
by secondary breast cancer
27th November 2023 by Sarah Thomas

The Advanced Breast Cancer International Consensus Conference in Lisbon takes place once every 2 years. It brings together medical experts from all over the world to share best practice in treating advanced and secondary breast cancer. This year our Research Manager, Dr Sarah Thomas, joined the conference virtually to catch up on all the latest scientific advances in the field. Read on as Sarah shares some of the highlights.
Two days of amazing science and ground-breaking clinical research is my cup of tea! The ABC conference is THE place to hear the latest developments in secondary breast cancer, and it’s easy to take part in the comfort of your own home via the livestream. After more than 50 inspirational talks, the sense of progress and passion for change was so clear. It’s hard to pick out highlights from such an incredible couple of days but here are a few things I learned:
The use of food supplements is sometimes called alternative or complementary medicine. We know that our diet plays an important role in our overall health and wellbeing, but there’s a lot of misinformation out there about cancer and food supplements. Dr André Dourado, Portugal, gave a helpful talk to explain how supplements interact with secondary breast cancer treatments.
One of the most important interactions between medication and the foods or supplements we take happens in the liver. Your liver breaks down nutrients in what you eat and removes harmful substances from your body. Some drugs need to be activated by liver enzymes in order to work, but there are many herbs and foods in our everyday diets that decrease the activity of these liver enzymes.
Here are a couple of examples of secondary breast cancer treatments that are broken down by liver enzymes:
This means that there are foods and supplements that may interact with these treatments.
What does this mean if you are on secondary breast cancer treatment? There are foods, teas and herbal supplements that can be beneficial and some that should be avoided. This depends on the type of treatment you are on. Good questions to ask your clinical team:
On the surface of a breast cancer cell, there are receptors that receive chemical signals in the body. These signals can be hormones or proteins that tell the cancer cells to grow.
‘HER2’ stands for ‘human epidermal growth factor receptor-2’. Non-cancerous cells have low levels of this receptor. Some breast cancers have too much, this is called HER2-positive (HER2+) breast cancer. Cancer is called HER2-negative (HER2-) if it has very low levels of HER2. But what about the people in the middle of the spectrum - are they HER2+ or HER2-?
This question has been a hot topic of debate in recent times, leading to the classification of a new subtype: HER2-low. Which still begs the question: if HER2 is on a scale from high to low, how do we decide who is HER2+, HER2-low and HER2-? What happens to the people who are on the borderline? Are they falling through the cracks? Prof Frédérique Penault-Llorca, France, an expert in pathology, tackled these questions on HER2-low.
By looking at a sample of cells under a microscope, pathologists provide a HER2 score based on the levels of HER2 receptors present on the cell surface. This can be seen using a dye which changes colour if HER2 is present.
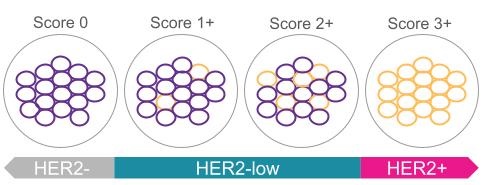
It’s very easy to tell the difference between HER2- and HER2+, and a test called an ISH assay is available to test the boundary between HER2-low (score 2+) and HER2+. However the boundary between HER2- (score 0) and HER2-low (score 1+) is less clear because the staining that can be seen under the microscope is at such a low intensity.
Another difficulty is that HER2 levels change over the course of treatment and can be found at different levels at different sites of metastasis.
What does this mean for treatment? As long as HER2-low has been recorded, either by biopsy or a surgical sample, treatments that target HER2 have been shown to be effective. People with the HER2- subtype should be reassessed over the course of treatment in case this changes to HER2-low over time, opening up other treatment options.
There is still a lack of targeted treatment options for triple negative breast cancer (TNBC) but hope is on the horizon. Prof Rebecca Dent, Singapore, shared the latest developments in new therapies for TNBC.
Right now the best approach for TNBC is to try to prevent it becoming metastatic through early and aggressive therapy, and to explore clinical trials at the earliest stage of secondary TNBC diagnosis.
One of the key points is that not all TNBC cases are the same, with varying levels of biomarkers, mutations and cell receptors, and different routes to diagnosis and early treatment. We are on the brink of molecular subtyping tests becoming much more readily available, which will crack open the possibilities for precision medicine for TNBC, allowing oncologists to move away from traditional chemotherapy towards treatment plans tailored to the individual based on targeted therapies.
A new type of treatment for TNBC, called an antibody-drug conjugate (ADC), is currently working its way through the clinical pipeline. Unlike traditional chemotherapy which can damage healthy cells, antibody drug conjugates are targeted medicines that deliver chemotherapy agents directly to where they are needed. They use an antibody that binds to a specific target on the cancer cell surface. After binding to the target, the chemotherapy drug is released into the cancer cell.
There are an amazing number of clinical trials currently underway exploring different antibody-drug conjugate treatments for TNBC and it’s really exciting to see the early findings from these studies. With the data from these trials, antibody-drug conjugates could rapidly become a first line treatment for TNBC in the future.
Prof Richard Sullivan, UK, delved into the complexities of cancer care amidst war.
A member of the audience asked Prof Sullivan about the current situation in Gaza where there is now a complete halt to all cancer treatment. He explained the difficulties in getting basic medical supplies such as burn bandages, to where they are needed, and that currently it’s not possible to transport medicines there. Even if the conflict ended tomorrow, the devastating long term impacts for cancer patients will last for years.
The number of refugees is expanding dramatically and war is causing a huge shift in the demography of the global population. Right now there are 104 million people worldwide who have been forcibly displaced from their homes due to war and around ¾ of refugees have been displaced for at least 5 years.
The scale and longevity of this displacement is having a critical impact on cancer diagnosis and treatment. Previously infectious diseases, child and maternal mortality, were the major health concerns during conflict but in recent times this has suddenly shifted towards cancer and in particular breast cancer, in countries where cancer care has previously been excellent before war has broken out. This transition has happened so fast that humanitarian aid has yet to catch up and faces serious economic challenges due to the cost of delivering cancer care in conflict settings.
So what are the solutions? Right now cancer is not a core part of the strategy in humanitarian aid and this needs to change to deliver a basic package of cancer care during conflict. Furthermore, in countries who are hosting large numbers of refugees, cancer care for those people needs to be included in their national cancer control planning. Finally, good quality cancer care cannot be delivered in the midst of war. It goes without saying that the path to health can only be found through peace.